The Impact of COVID–19 on Oncology Pharmacy and Cancer Care: A Multi-
Country Cross-Sectional Study- new title
Authors:
Maja Kuzmanovic, Agnieszka Bienert, Antonina Kokisheva, Marianna Veraldi, Paul Andreianu, Klaus Meier
Abstract
Introduction:
The COVID–19 pandemic profoundly disrupted healthcare systems worldwide, necessitating rapid adaptations in oncology service delivery to reduce infection risks and preserve hospital capacity. This study aimed to assess healthcare professionals’ perceptions of how oncological care and the oncology pharmacy workforce were affected during the pandemic.
Methods:
The ESOP Global Working Group on COVID–19 developed a 21-item cross-sectional online survey exploring changes in oncological therapy, palliative and preventive care, communication, workplace environment, and preparedness for future crises. The survey was translated into nine languages and distributed between April and July 2024 among ESOP Global members. Responses were analysed descriptively, with results presented as n/N (%) and 95% confidence intervals (Wilson method).
Results:
A total of 286 valid responses were received from five world regions. Most participants were employed in general hospitals (55.1%) or oncology centres (23.3%), and 74.7% reported more than ten years of oncology experience. Reported impacts included protocol modifications in curative therapy (58.3%), disruptions in palliative care (46.5%) and preventive services (62.9%), and exposure to verbal or psychological abuse (23.6%). Only 20.5% of respondents reported having received structured crisis management training, while 63.5% perceived improved system preparedness following the pandemic.
Conclusion:
The findings indicate that oncology pharmacy professionals faced substantial operational and psychosocial challenges during the COVID–19 pandemic, while also demonstrating resilience, adaptability, and innovative practice changes. The pandemic accelerated digital transformation and strengthened interdisciplinary collaboration, highlighting the importance of structured crisis preparedness training and institutional support to ensure sustainable and resilient oncology services during future public health emergencies.
Keywords:
COVID–19 pandemic; oncology care; oncology pharmacy; healthcare professionals; palliative care; mental health; pandemic preparedness
Introduction
The COVID–19 pandemic has posed an unprecedented challenge for healthcare systems around the world, with significant impacts on the delivery of healthcare services and, in particular, oncological care. The restrictions imposed to limit the spread of the SARS-CoV–2 virus, such as the reduction of hospital resources and the need to protect patients and healthcare workers from infection, have inevitably affected the management of patients suffering from oncological diseases.
This evidence underlines the need for an in-depth reflection on the strategies to be adopted to ensure the continuity and effectiveness of oncological care even in health emergency situations. The pandemic has, in fact, highlighted the vulnerability of cancer patients and the need to implement resilient care models, capable of quickly adapting to crisis scenarios.
It is hoped that the results of scientific research and the experiences gained during the pandemic will help guide health policies and promote an integrated and multidisciplinary approach in the management of cancer patients, with the aim of guaranteeing them the best possible care, even in times of crisis.
In this context, scientific research has taken action to fully understand the impact of the pandemic on oncological care. Numerous studies, conducted globally, have shown how the health emergency has led to delays in diagnoses, interruptions in treatment and difficulties in accessing care for cancer patients.
Some critical aspects that emerged from the studies are:
Delays in diagnosis and excess deaths: A study published in Journal of Clinical Oncology (1) estimated that there were approximately 100,000 excess cancer deaths in the United States due to delays in treatment during the pandemic.
Impact on care pathways: Research conducted in Italy and published in The Lancet Oncology (2) found that 40% of cancer patients have experienced delays or changes in their treatment pathway due to the pandemic.
Difficulty in accessing care: A further study (3) analysed the impact of the pandemic on cancer care in the United States, highlighting delays in diagnoses, interruptions in treatment, and difficulties in accessing care for cancer patients.
Global impact and long-term implications: A series of articles (4) explored several aspects of the impact of the pandemic on cancer care, including the management of cancer patients during the pandemic, the impact on clinical trials, and the long-term implications for patients and health systems. Several studies (5) have summarised the results of numerous studies on the impact of the pandemic on cancer care, confirming the evidence of delays in diagnosis, interruptions in treatment and difficulties in accessing care.
Comprehensive overview and challenges: Further research (6) has provided a comprehensive overview of the impact of the pandemic on cancer care, exploring the challenges faced by patients, health systems and cancer research.
These data, together with the direct testimonies of healthcare professionals, underline the importance of deepening the understanding of the impact of COVID–19 on cancer care, in order to improve patient management and ensure continuity of care even in health emergency situations. The articles cited help us understand how this pandemic “storm” has affected the care of cancer patients, who are particularly vulnerable.
The increase in the time to get a cancer diagnosis and the difficulties in regularly following therapies have happened for several reasons such as:
•the fear of contagion: many patients have avoided going to the hospital for fear of contracting the virus, thus delaying any checks or tests;
•hospital overload: at many times, healthcare facilities have been focused on managing COVID–19 patients, resulting in reduced resources available for other conditions, including cancer;
•restrictions and lockdowns: travel restrictions and closures of some businesses have made it more difficult for patients to reach healthcare facilities and follow treatments.
In addition to the more “practical” aspects, the pandemic has had a strong psychological impact on cancer patients. Many have experienced the period of illness with greater anxiety and stress, feeling even more vulnerable and worried about the future (7).
Healthcare personnel have also suffered a lot of stress during the pandemic. Doctors and nurses have found themselves having to manage an increase in work, the fear of contagion, the need to reorganise treatment pathways and, in some cases, the difficulty in providing adequate support to patients.
The pandemic has also had an impact on cancer research. Many clinical trials have been halted or slowed down, with possible negative consequences for the development of new therapies. (8)
The articles indicated show us how the pandemic has put a strain on cancer care, with consequences for both patients and healthcare personnel. It is essential that, once the emergency is over, this experience is treasured to improve the organisation of health systems and ensure that cancer patients always receive the best care, even in crisis situations.
In this context, it becomes essential to understand how healthcare professionals who work daily in contact with cancer patients have experienced and interpreted these changes. A survey aimed at assessing their individual perspectives can provide valuable insights into the real impact of the pandemic on cancer care and the challenges facing the healthcare system.
In fact, the aim of this survey was to assess individual perspectives of cancer care by healthcare staff on changes in oncological care due to COVID–19.
Methods and materials:
A web-based 21-item survey was formulated by a working party of the ESOP Global Special Interest Working Group (WG) on COVID - 19 (appendix 1), based on literature review and expert consensus.The survey consisted of various topics on the impact of the Covid–19 pandemic on oncological care, healthcare worker and preparing for new pandemic(s) and has been translated into 9 languages using a forward-backward process, verified by bilingual oncology pharmacists. The survey was set up in LamaPoll (LamaPoll, Berlin, Germany) and checked for technical accuracy and understandability by five members of the Special Interest Group to ensure clarity and technical accuracy. All ESOP Global members were asked to participate via a dedicated email newsletter and participation in the survey constitutes consent to the processing of data. As the total number of recipients cannot be reconstructed, response rate and potential non-response bias could not be calculated; this is acknowledged as a limitation. The time to complete the survey was estimated to be 10–15 minutes. Eligibility criteria included age ≥18 years and active participation in oncological care. The survey was open online from April to the end of July 2024. Results were exported to Excel (Microsoft Office 2016, Microsoft, Redmond, USA) and analysed using descriptive statistics Results are expressed as n/N (%) with 95% confidence intervals (Wilson method).
This study did not require ethical approval, as it collected only anonymous professional data. Participation was voluntary, and informed consent was implied by survey completion. Data handling complied with EU GDPR (2016/679).
Results:
The survey data was collected from 286 respondents (61.7% of respondents confirmed their ESOP membership), reaching a total of five regions of the world: Africa, America, Asia, Europe and Australia/Oceania.
The majority of respondents reported being employed in general hospitals (55.1%) or specialised oncology centres (23.3%). Furthermore, a significant proportion (74.7%) had more than ten years of experience in their respective professional fields, indicating a high level of expertise within the study sample (Fig.1, Fig. 2).
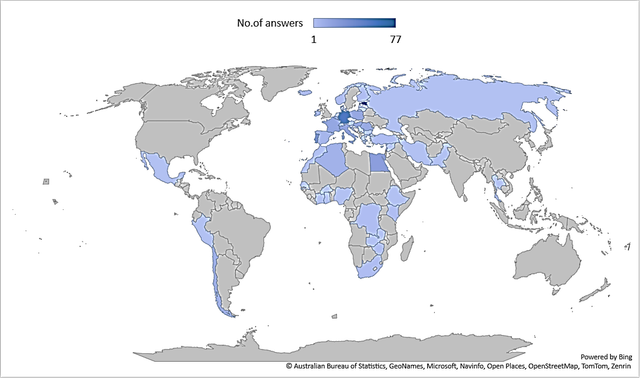
Fig. 1 Countries participating in the survey
Fig. 2 Primary workplace of respondents
Fig. 3 Perception of impact on professional development(Q:
How do you think the COVID–19 pandemic has impacted your professional career?)
Fig. 4 Job titles of respondents
Despite the COVID–19 pandemic lasting over four years, healthcare professionals report varied perceptions of its impact on their careers. Around one-third (35.9%) stated it had no significant effect on their professional development, while 30.4% perceived a positive impact and 33.7% reported a negative one (Fig. 3). These results highlight the complexity of individual experiences and the need to explore both personal and systemic factors influencing professional trajectories.
Positive outcomes included improved knowledge and skills, expanded responsibilities, and engagement in advisory bodies and working groups addressing the pandemic. Nearly half of respondents participated in multidisciplinary teams, contributing to more effective pandemic management and evidence-based infection control strategies.
Given that most respondents were pharmacists or pharmaceutical assistants (87.7%), with fewer physicians (5.0%) and nurses (0.8%), the findings confirm the successful integration of various healthcare professionals into collaborative, team-based COVID–19 response efforts.
Fig. 5 Perception of impact on curative oncology therapies(Q:
Did the COVID 19 pandemic cause changes in curative therapy for oncology patients?)
An inquiry into the impact of the COVID–19 pandemic on curative oncological therapies revealed that 58.3% of respondents reported partial, temporary, or complete alterations in treatment protocols, whereas 41.7% indicated no such changes occurred (Fig.5).
Fig. 6 Changes in palliative care(Q:
Did the COVID 19 pandemic cause changes in palliative care for oncology patients?)
The pandemic’s influence on palliative care services, including the accessibility of multidisciplinary support teams, was also evaluated. According to the findings, 46.5% of participants observed disruptions in the provision of palliative care-ranging from partial to complete-while 53.5% did not notice the impact of COVID on this area (Fig. 6).
Fig. 7 Modifications in preventive oncology
(
Q:
Did the COVID 19 pandemic cause changes in prevention for oncology patients?)
Comparable trends were identified in responses regarding preventive oncology services. A total of 62.9% of respondents reported partial, temporary, or complete modifications in preventive care during the pandemic, while 37.1% noted no significant changes (Fig. 7).
Fig. 8 Adequacy of palliative care teams(Q:
Did you have enough support teams for patients receiving palliative care?)
According to the results, 30.7% of respondents believed that palliative care support teams were adequate, while 32.4% reported inadequacy. A notable proportion of participants (37.0%) indicated that the question was not applicable to their context. (Fig. 8)
Fig. 9 Conflicting opinions among professionals(Q:
Has the COVID–19 pandemic caused a conflict of opinion among healthcare workers at your place of work?)
Fig. 10 Perception of impact on communication(Q:
How did the COVID–19 pandemic impacted the communication between healthcare professionals and patients?)
Moreover, the pandemic appeared to negatively affect communication and collegiality among healthcare workers, with 57.5% reporting conflicting opinions and 41.6% indicating impaired communication (Fig. 9, Fig.10).
Workplace abuse was also a notable concern during the pandemic. A total of 23.6% of respondents reported experiencing abuse at work, with approximately 70% of these cases involving verbal (36.5%) or psychological abuse (35.7%) (Table 1, Fig. 11).
Table 1. Perceived organizational improvements, crisis training and preparedness.
| Yes | No |
Workplace Abuse During COVID–19 | 23.6% | 76.4% |
| ||
Training Received for Managing Critical Situations | 20.5% | 79.5% |
| ||
Staff Readiness for Future Pandemic | 63.5% | 36.5% |
Fig. 11 Types of workplace abuse
(
Q:
What type of workplace abuse were you exposed to? (multiple answers))
Only 20.5% of healthcare workers reported having received training on how to manage critical situations, highlighting a significant gap in preparedness. The vast majority (79.5%) indicated that they had not received any such training, underscoring the need for structured educational programs and institutional support in future crisis scenarios (Table 1).
The majority of respondents (63.5%) indicated that the COVID–19 pandemic has contributed to strengthening the healthcare system’s preparedness for future public health crises. Conversely, 36.5% did not perceive any improvement, highlighting the need for continued investment in system resilience, infrastructure, and strategic planning.
Fig. 12 Perceived positive and negative organisational changes during the COVID–19 pandemic(Q:
What changes to multiple professional team working will you maintain? (multiple answers))
Reported changes in work organisation among healthcare workers are illustrated. The most frequently reported positive change was the introduction of hybrid working models (62.7%), followed by the elimination of printed paperwork (31.9%), adequate preparation time (31.1%), and streamlining of cases (30.3%). However, 35.2% of respondents indicated reduced opportunities for professional development as a negative impact, while 10.5% reported no noticeable organisational changes. A smaller proportion selected “Other” (2.4% and 3.1%) or “None” (7.7%). These findings highlight a shift toward digital and flexible working practices, while also emphasising the need to address professional development gaps that emerged during the pandemic (Fig.12).
Fig. 13 Perceived organizational and digital improvements(Q:
What changes provided solutions? (multiple answers))
Overall, reduced travel time enabled by virtual access (19.9%) emerged as the most frequently recognised benefit of remote and digital work practices during the COVID–19 pandemic. Other notable advantages included enhanced IT infrastructure (17.8%), a more streamlined approach to virtual meetings (17.8%), and improved availability and attendance of clinicians (17.5%). Respondents also reported the availability of multidisciplinary team guidelines (10.7%), increased opportunities for continuous professional development (8.9%), and greater continuity of care (6.3%). Only a small proportion (1.2%) indicated that no benefits were observed (Fig. 13)
Discussion
This study provides a comprehensive analysis of the multifactorial impact of the COVID–19
pandemic on healthcare professionals involved in oncological care, with particular emphasis on
the roles and experiences of pharmacists and pharmaceutical assistants. The respondent
profile—predominantly individuals employed in general hospitals or specialised oncology
centres (Fig. 2), over 75% with more than a decade of professional experience-supports the
credibility of the data and strengthens the generalisability of insights across a mature
professional demographic. These findings align with existing literature highlighting the pivotal
role of experienced healthcare workers in maintaining continuity and quality of care during
large-scale health emergencies (9,10).
A notable feature of the study is the heterogeneous perception of the pandemic's impact on
professional trajectories. While about one-third of respondents reported minimal effects, others
experienced either positive or negative consequences, suggesting that the pandemic functioned
both as a disruptor and as a catalyst depending on individual and contextual factors (Fig. 3). This
variability reflects the complex interplay between personal resilience, institutional support, and
broader systemic challenges, which together shape professional adaptation during prolonged
crises (11,12). Several participants also highlighted constructive outcomes, such as acquiring
new clinical competencies, taking on expanded responsibilities, and engaging in
multidisciplinary advisory panels, consistent with international reports recognising the essential
role pharmacists played in pandemic response efforts (13).
The pandemic caused significant disruptions in the continuum of oncological care. Over 60% of
respondents reported changes or suspensions in preventive oncology services, and nearly half
noted substantial interruptions in palliative care—often compounded by limited access to
specialised support teams (Fig. 6–8). These observations mirror global evidence of delayed
cancer screenings, postponed diagnostics, and the reallocation of oncological resources, which
collectively compromised optimal cancer management and increased patient vulnerability
(14,15). Shifting priorities within healthcare systems highlighted structural weaknesses and
underscored the importance of adaptable care pathways that preserve oncological services even
during public health crises.
Professional dynamics and interpersonal relationships were similarly affected. More than half of
participants reported impaired communication and increased interprofessional conflict,
indicating that heightened pressure and evolving care protocols strained established collaborative
frameworks (Fig. 10). Workplace abuse—predominantly verbal and psychological—was
reported by a notable proportion of healthcare workers (Fig. 12), yet only a minority had
received training to manage such incidents, revealing gaps in institutional preparedness and
support (Table 1). These findings are consistent with literature documenting increased
occupational violence during the pandemic and reinforce the urgent need for staff protection
policies, mental health support, and organisational accountability mechanisms (17,18).
Despite these challenges, respondents identified several pandemic-induced structural
improvements. Rapid adoption of hybrid working models, widespread digitalisation of clinical
documentation, and streamlined administrative workflows were frequently viewed as beneficial
developments that may persist beyond the pandemic (Fig. 12). Concerns remain, however,
regarding fragmentation of patient information, reduced depth of patient-clinician interactions,
and limited in-person mentorship and professional development opportunities. In response,
adaptive strategies such as enhanced IT infrastructure, development of multidisciplinary
guidelines, and strengthened continuing professional education were implemented, reflecting the
resilience and innovation capacity of the healthcare sector (Fig. 13, 19).
Limitations and Contextualization
This study has several limitations. A non-probability convenience sample was used, which may
introduce selection bias, and the response rate could not be reconstructed. Recall bias is possible,
as the survey conducted in 2024 captured experiences from 2020–2023; as a cross-sectional
study, it cannot assess temporal changes. Additionally, the questionnaire lacked formal
psychometric validation and full cross-cultural adaptation. Despite these limitations, the study
offers valuable late-pandemic insights into the experiences of the oncology pharmacy workforce,
complementing evidence from large initiatives such as the CCC19 cohort. These findings should
be interpreted with caution, but they provide a meaningful contribution to understanding
workforce challenges, innovations, and lessons learned for future public health crises.
Conclusion:
The COVID–19 pandemic significantly disrupted oncological care, exposing vulnerabilities in
prevention, palliative services, and workplace conditions while increasing psychological stress
among healthcare professionals. Nevertheless, the oncology pharmacy workforce demonstrated
remarkable adaptability through the rapid adoption of digital tools, hybrid work models, and
improved workflow efficiency. The coexistence of these challenges and innovations highlights
both systemic weaknesses and the profession’s resilience. To enhance future preparedness,
healthcare institutions must prioritise structured crisis training, psychological support, and ethical
guidance frameworks, particularly in palliative and end-of-life care. Strengthening
interprofessional collaboration and integrating digital solutions into oncology pharmacy practice
will be essential to build sustainable and resilient cancer care systems capable of withstanding
future public health crises.
Ethical Considerations
Informed consent
Participation in the study was voluntary and anonymous. By completing the online questionnaire,
participants provided implied informed consent to participate. Prior to starting the, questionnaire, an introductory statement clearly explained the study’s purpose, the voluntary nature of participation, and the option to withdraw at any time without consequences.
Data protection
All collected data were fully anonymized and stored securely in password-protected files
accessible only to the study investigators. No identifiable personal information was collected.
The study complied with applicable data protection regulations, including the EU General Data
Protection Regulation (GDPR, Regulation (EU) 2016/679). Data were analysed and reported
exclusively in aggregate form to ensure confidentiality.
Declarations
Funding
This research received no specific grant from any funding agency in the public, commercial, or
not-for-profit sectors.
Conflict of interest
The authors declare no potential conflicts of interest related to this study.
Data availability
The datasets generated and analysed during the current study are available from the
corresponding author upon reasonable request.
References:
Zhao J, Han X, Miller KD, Zheng Z, Nogueira L, Islami F, et al. Association of the COVID–19 pandemic and changes in patterns of cancer-related mortality in the United States. JCO Oncol. Pract. 2023 Jul;19(7):501–8. doi: 10.1200/OP.22.00522. PMID: 37040580.
Ambroggi M, Citterio C, Vecchia S, Riva A, Mordenti P, Cavanna L. Impact of the COVID–19 pandemic on the oncologic activities (diagnosis, treatment, clinical trials enrolment of a general hospital in a district with high prevalence of SARS-COV–2 in Italy. Support Care Cancer. 2022 Apr;30(4):3225–31. doi: 10.1007/s00520–021–06667-y. PMID: 34977981; PMCID: PMC8720559.
Richards M, Anderson M, Carter P, Ebert BL, Mossialos E. The impact of the COVID–19 pandemic on cancer care. Nat Cancer. 2020 Jun;1(6):565–7. doi: 10.1038/s43018–020–0074-y. PMID: 35121972; PMCID: PMC7238956.
Kuderer NM, Choueiri TK, Shah DP, Shyr Y, Rubinstein SM, Rivera DR, et al. Clinical impact of COVID–19 on patients with cancer (CCC19): a cohort study. Lancet. 2020 Jun 20;395(10241):1907–18. doi: 10.1016/S0140–6736(20)31187–9. PMID: 32473681; PMCID: PMC7255743.
Jazieh AR, Akbulut H, Curigliano G, Rogado A, Alsharm AA, Razis ED, et al. Impact of the COVID–19 pandemic on cancer care: A global collaborative study. JCO Glob. Oncol. 2020 Sep;6:1428–38. doi: 10.1200/GO.20.00351. PMID: 32986516; PMCID: PMC7529504.
Moujaess E, Kourie HR, Ghosn M. Cancer patients and research during COVID–19 pandemic: A systematic review of current evidence. Crit. Rev. Oncol. Hematol. 2020 Jun; 150:102972. doi: 10.1016/j.critrevonc.2020.102972. PMID: 32344317; PMCID: PMC7174983.
Tsamakis K, Gavriatopoulou M, Schizas D, Stravodimou A, Mougkou A, Tsiptsios D, Sioulas V, Spartalis E, Sioulas AD, Sfikakis PP, Dimopoulos MA, Rizos E. Oncology during the COVID–19 pandemic: challenges, dilemmas, and the psychosocial impact on cancer patients. Cancer Treat Rev. 2020 Sep; 88:102111. doi: 10.1016/j.ctrv.2020.102111. Epub 2020 May 29. PMID: 32502711; PMCID: PMC7285823.
Bardet A, Fonseca A, Lambert G, Tinquaut F, Lievre A, Morin M, Mollevi C, Trone JC, Bousquet G, Mornex F, Campion L, Dufresne A. Impact of COVID–19 on healthcare organisation and cancer care: a systematic review. Cancer Treat Rev. 2021 Aug; 99:102289. doi: 10.1016/j.ctrv.2021.102289. Epub 2021 Jul 1. PMID: 34218158; PMCID: PMC8213441.
9. Liu Q, Luo D, Haase JE, Guo Q, Wang XQ, Liu S, et al. The experiences of health-care providers during the COVID–19 crisis in China: a qualitative study. Lancet Glob. Health. 2020 Jun;8(6):e790–8. doi: 10.1016/S2214–109X(20)30204–7. PMID: 32573443; PMCID: PMC7190296.
10. McMahon DE, Peters GA, Ivers LC, Freeman EE. Global resource shortages during COVID–19: Bad news for low-income countries. PLoS Negl Trop Dis. 2020 Jul;14(7):e0008412. doi: 10.1371/journal.pntd.0008412. PMID: 32628664; PMCID: PMC7337278.
11. Kisely S, Warren N, McMahon L, Dalais C, Henry I, Siskind D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: rapid review and meta-analysis. BMJ. 2020 May 5;369:m1642. doi: 10.1136/bmj.m1642. PMID: 32371466; PMCID: PMC7199468.
12. Shanafelt T, Ripp J, Trockel M. Understanding and addressing sources of anxiety among health care professionals during the COVID–19 pandemic. JAMA. 2020 Jun 2;323(21):2133–4. doi: 10.1001/jama.2020.5893. PMID: 32259193.
13. Visacri MB, Figueiredo IV, Lima TM. Role of pharmacist during the COVID–19 pandemic: A scoping review. Res. Social Adm. Pharm. 2021 Jan;17(1):1799–806. doi: 10.1016/j.sapharm.2020.07.003. PMID: 33317760; PMCID: PMC7334137.
14. Patt D, Gordan L, Diaz M, Okon T, Grady L, Harmison M, et al. Impact of COVID–19 on cancer care: How the pandemic is delaying cancer diagnosis and treatment for American seniors. JCO Clin. Cancer Inform. 2020 Nov;4:1059–71. doi: 10.1200/CCI.20.00134. PMID: 33253013; PMCID: PMC7713534.
15. Maringe C, Spicer J, Morris M, Purushotham A, Nolte E, Sullivan R, et al. The impact of the COVID–19 pandemic on cancer deaths due to delays in diagnosis in England, UK: a national, population-based, modelling study. Lancet Oncol. 2020 Aug;21(8):1023–34. doi: 10.1016/S1470–2045(20)30388–0. PMID: 32679067; PMCID: PMC7367663.
16. Yorke AM, Smith LM, Mostrom E. The impact of COVID–19 on interprofessional collaborative practice through the lens of acute care physical therapists: A case series. J Acute Care Phys Ther. 2023 Apr;14(2):93–103. doi: 10.1097/JAT.0000000000000208. PMID: 36968179; PMCID: PMC10032220.
17. Gascón S, Leiter MP, Stright N, Santed MA, Montero-Marín J, Andrés E, et al. A factor confirmation and convergent validity of the “areas of worklife scale” (AWS) to Spanish translation. Health Qual. Life Outcomes. 2013 Apr 18;11:63. doi: 10.1186/1477–7525–11–63. PMID: 23596987; PMCID: PMC3637316.
18. Taylor S, Landry CA, Paluszek MM, Fergus TA, McKay D, Asmundson GJG. COVID stress syndrome: Concept, structure, and correlates. Depress Anxiety. 2020 Aug;37(8):706–14. doi: 10.1002/da.23071. PMID: 32627255; PMCID: PMC7362150.
19. Whitelaw S, Mamas MA, Topol E, Van Spall HGC. Applications of digital technology in COVID–19 pandemic planning and response. Lancet Digit. Health. 2020 Aug;2(8):e435–40. doi: 10.1016/S2589–7500(20)30142–4. PMID: 32835201; PMCID: PMC7324092.
Appendix
COVID–19 SURVEY
1. Are you ESOP Global member?
a) Уes
b) No
2. Please choose your country: (drop-down list)
3. How many years of work experience do you have?
a) <5 years
b) 6–10 years
c) >10 years
4. What is your primary place of work?
a) Cancer Centre (cancer patients only)
b) General Hospital (cancer patients and other specialties)
c)Private outpatient clinic
d) Pharmaceutical/biotechnology company
e) Healthcare organization
f) Community Pharmacy
g)Laboratory
h) Other (text field to mention the other place of work)
5. Job title
a)Physician
b)Pharmacist
c)Nurse
d)Pharmaceutical assistance
e)Other, please specify: (text field to mention the job title)
6. How do you think the COVID–19 pandemic has impacted your professional career?
a)Positively
b) No impact.
c) Negatively
7. Have you been invited to join any advisory committee/group focused on COVID–19 management?
(You can select multiple answers)
a)No
b)Yes, at the hospital level
c)Yes, at the regional level
d)Yes, at the national level
e)Yes, at the international level
8. Did the COVID 19 pandemic cause changes in curative therapy for oncology patients?
a) Not at all
b) Partial / temporary changes, how? __________
c) Completely, how? __________
9. Did the COVID 19 pandemic cause changes in prevention for oncology patients?
a) Not at all
b) Partial / temporary changes, how? __________
c) Completely, how? __________
10. Did the COVID 19 pandemic cause changes in palliative care for oncology patients?
a) Not at all
b) Partial / temporary changes, how? __________
c) Completely, how? __________
11. Did you have enough support teams for patients receiving palliative care?
a) Yes
b) No
c) Not applicable.
12. Has the COVID–19 pandemic caused a conflict of opinion among healthcare workers at your place of work?
a)Yes
b)No
c)I do not know
13. How did the COVID–19 pandemic impacted the communication between healthcare professionals and patients?
a) Negative impact
b) No impact
c) Positive impact
14. How do you think the COVID–19 pandemic has impacted your role?
a)Positively
b) No impact.
c) Negatively
15. Were you subject to any exposure to abuse at your workplace during Covid–19 pandemic?
a)Yes—please continue with Q16
b)No—please skip Q16
16. What type of workplace abuse were you exposed to (multiple answers)::
a)physical abuse
b)verbal abuse
c) psychological abuse
d) discrimination
e) other
17. Have you received any training on how to deal with workplace abuse?
a)Yes
b)No
18. What changes to multiple professional team working will you maintain? (multiple answers)
a)Hybrid working.
b)Streamlining of cases
c)No printed paperwork
d)Adequate preparation time
e)Other (any commentary)
f)None.
19. Have changes caused any specific problems? (multiple answers)
a)IT- related issues and slower meeting, longer lists and delays
b)Issues with virtual meetings
c)Quality of patient related information
d)Issues around meeting room space
e)Adjustment period to virtual/hybrid working
f)Increased caseload and complexity of patients
g)Reduced opportunities for professional development.
h) Other (any commentary)
i) None.
20. What changes provided solutions? (multiple answers)
a)Virtual meetings and increased attendance /availability of clinicians
b)Improved IT infrastructure.
c)Virtual meetings streamlined approach
d)Virtual access reduced travel time
e)Continuity of care
f)Multi Professional Team guidelines available
g)Continuous Professional Development
h)None
21. Based on the lessons learned, if a new pandemic will be declared soon, do you feel prepared for it?
a)Yes
b)No
Summary
shivam
Metadata
Test Abstract for crossRef
2024
1
1